
Page Title
Autumn 2020
Welcome to the 2020 Autumn Edition of the Nurse & Midwife Newsletter. In this edition we look at a core part of nursing and midwifery — death, dying and grief.
We have brought together a really broad range of resources to help people at all stages of career and particularly in line with current events.
WARNING: This edition deals with a range of sensitive issues and may be triggering for some readers.
Death, Dying and Grief – through a pandemic and beyond
Releasing this edition of the newsletter during a pandemic was difficult decision for everyone at Nurse & Midwife Support. Mark explains why we have and how we think it will help. Read more.
Confronted by grief: How to function in the face of death
All nurses and midwives will witness death. The Nurse & Midwife Support team offer tips to help you navigate the experience. Read more.
New Resources: Death dying and grief + Vicarious trauma
We look at how Death dying and grief and Vicarious trauma affects nurses and midwives and resources that are available to help you cope.
Field notes on death
A beautiful and poignant story written by a nurse, witnessing and caring for people while dying and in death. Read more.
Babies born still
A beautiful birth, with a baby born still marked new beginnings for this couple and their photographer, read their powerful story. Read more.
How to enjoy life in the presence of death
Palliative care nurse Carole Arbuckle explains how she learned that self-care is the key to coping with the complexity of grief and loss. Not just ‘pushing through’. Read more.
Podcast: Death, Dying & Grief
Nurses and Midwives aren’t immune from the effects of grief, compassion fatigue and vicarious trauma. Mark discusses those effects with guests Lea McInerney and Carole Arbuckle in this new episode of our podcast. Read more.
by Mark Aitken

Welcome to the Autumn 2020 Edition of the Nurse & Midwife Support newsletter.
In this edition we look at the complexities of dealing with death, dying and grief, an intrinsic part of being a nurse and midwife. This subject may feel more raw than usual as we deal with ongoing widespread drought, the fallout of this summer’s bushfires, and now we find ourselves in the grip of a pandemic.
Is it the right time for this newsletter?
This edition has been planned for over 12 months. In light of the current situation we seriously considered whether to defer it until another time. Collectively, we are already experiencing grief and expect that harder times are to come. We didn’t want to place additional stress on a group that are already shouldering quite a burden.
However, putting out new resources that may help even one nurse or midwife deal with this complex issue — during a very high stress period — felt like the right thing to do. If we can give any of you additional resilience to work through this, without relying on unhelpful coping strategies, all of us will be in a better place. After all, healthy nurses and midwives mean better outcomes for patients.
So after careful deliberation we came to the decision that this edition was more important now than ever.
We hope that you find this newsletter really helpful and want to remind you all that we are here to help support you. It’s always a good time to call us — after any shift, on a bad day, even just to hear a voice that understands what you are going through. Call us 1800 667 877.
If you aren’t ready
If it doesn’t feel like the information in this newsletter would be helpful for you at the moment, please don’t read it. Take some time away and do other things that bring you joy. When you are ready we will still be here. In fact, we recommend you also do this with social media and the news as well. If it is making you feel more stressed, take a rest from it.
Asking for support as a carer
Already this year I have heard story after story of the capacity of people to pick themselves up and keep going, which is an incredible testament to the strength of our communities. At the same time, we need to recognise how important it is not only to offer support but to ask for it too.
Nurses and midwives care for others when they are at their most vulnerable, and care for those who are dying. We bear witness to death and support those who are grieving. We often do this on the back of our own experiences of death, loss and grief. Mostly, we manage the emotions we experience, but at times it can feel like we are overloaded by death and grief. We might feel that we are running on empty and need a moment to replenish and self-soothe — but on we go, because we have another person to care for and support.
Grieving with our patients and their families
Nurses and midwives play a pivotal role in supporting people when they are dying. We are intimately involved with their grief and death, and the grief of their loved ones, sometimes in sudden or traumatic circumstances. While this is part of the work of nurses and midwives it may take a toll on our emotional wellbeing and enjoyment of life.
There is research that confirms nurses and midwives grieve for those who they care for who have died. However, we may not fully understand or recognise our emotional responses, particularly if we are fatigued or stressed. Many nurses and midwives tell us they feel unprepared or unequipped to manage their reactions. It is common for nurses or midwives to not seek support and “push through” until a distressing psychological issue emerges or until someone else notices and intervenes.
Taking the first step
The first step to prevent this occurring is awareness and early intervention. Awareness of the risks and support available aids resilience and reduces the risk of burnout and compassion fatigue. Work-life balance, self-care strategies, and communication skills are vital for emotional and professional well-being and growth. Now, more than ever we encourage you to take the time to prioritise these strategies.
If you would like to know more, or are concerned about your feelings, you can call our confidential support line 24/7 on 1800 667 877 or access our website resources.
It’s Ok to ask for support — indeed, it is vital. Your health matters.
Mark Aitken RN
Stakeholder Engagement Manager
Nurse & Midwife Support
By Nurse & Midwife Support Clinicians

All nurses and midwives will witness death. The Nurse & Midwife Support team offer tips to help you navigate the experience.
As nurses and midwives, we are privileged to witness the beginning and end of the lives of people we care for in a professional and personal sense. Sometimes, people die peacefully and we see both sadness and relief. Sometimes they die in chaos and we are left with the lingering terror and confusion of their death.
An appropriate level of grief
As professionals, we often have unrealistic expectations of ourselves. We think we need to be strong and mask our emotions in the face of a patient’s death. That is not necessarily the healthiest, nor the most helpful reaction. It is ok to feel sad or cry with family and loved ones. Many people find it both affirming and helpful to express feelings of loss as it is an example of our shared humanity.
However it is important to remember that it is not ok to be so upset that they need to comfort you in the midst of their grief. If you feel that this is a possibility try to remove yourself from the situation, talking to your manager about having particular triggers may be helpful.
Sometimes it hits harder than others
Sometimes, the grief hits harder than normal. Maybe the person who died reminds you of someone you loved. Maybe they’re so young that their death feels unfair or premature. Maybe you just really liked them. You also might be reeling from the cumulative effect of multiple deaths in a short time.
At times like this, it’s possible you might recognise in yourself a profound reaction that feels extreme — or the opposite. You might feel jaded, cold and unaffected in a way that feels unnatural. Either way, it’s helpful to seek support from peers, pastoral care, an employee assistance program, or Nurse & Midwife Support.
Taking a step to recognise your feelings contributes to your emotional health. Self-care helps you to replenish your caring resources so you can continue to help your patients and your families through these difficult moments.
Under ‘normal’ hospital circumstances, The Nurse & Midwife Support clinician team suggested a range of strategies to help people in the immediate aftermath of the death of a loved one:
- Ask if there is anybody you could ring on their behalf.
- Offer to gather and pack belongings and personal items.
- Ask if they would like to help wash and prepare the person.
- Be mindful of their cultural and spiritual needs — everybody grieves differently.
- Listen.
- Offer space, respect, and privacy.
Some of these strategies will need to change in the circumstances of COVID-19. Many will find it confronting to deny people the opportunity to visit a dying loved one. Even if you’re not a believer, the serenity prayer can be helpful here:
Grant me the serenity to accept the things I cannot change, the courage to change the things I can, and the wisdom to know the difference.
You don’t have the power to make it safe for people to visit their loved ones in hospital right now, but you do have the power to protect them by enforcing new guidelines around visitation. You are doing everything you can to honour your patient by protecting their loved ones.
Focus on the things you can do, and forgive yourself for the things that you can’t.
Taking a moment
If you’re struggling, it’s important to take a moment to attend to your own grief. Do something easy and automatic: make a cup of tea, focus on a breathing exercise, or apply some hand cream in a mindful manner. Consider calling a friend or NM Support when you get home. Treating yourself with kindness will help to ensure you have the strength to ensure your patients’ families are well cared for in their time of grief.
Death is something all nurses and midwives will be affected by in their careers. If you need to talk, we’re here: call Nurse and Midwife Support 24/7 on 1800 667 877 or email us.
by Lea McInerney

Originally published in Griffith Review 41: Now We Are Ten, July 2013
Introduction from Mark Aitken
I read a lot of research papers, articles and stories while compiling the Death, dying and grief webpage and newsletter. This piece stood out, it is a beautiful and poignant story written by a nurse, witnessing and caring for people while dying and in death.
I think that it will resonate with many nurses and midwives, validating their own experiences and emotions. It is our privilege to share it with you, with the very kind permission of Lea. I hope that you enjoy it as much as I do every time I read it. You can also hear Lea discuss this memoir and other issues related to death dying and grief on this episode of our podcast.
I was in a foul mood a few weeks back. In a flash of bleak insight, I wrote on a scrap of paper: I hope I don't die today, this would be a very bad mood to die in.
When I was a small child, death was a regular event in my life, mostly as performance and play. My numerous siblings and I would line up, the current toddler in a bulky nappy waddling along at the back, ready to bury yet another mouse or a bird found in the bush near our home. With undiluted Irish Catholic ancestry, ritual was thick in our blood. We would proceed from the backyard, along the side veranda, down to the front garden, one of us carefully carrying the shoe box with the little body laid on leaves and grass cuttings, one carrying a cross made from two Popsicle sticks, one conducting the service at the graveside. I remember it now as big on ceremony and small on feeling.
My first awareness of death as personally wounding came when I was eight. ‘Senator Kennedy has been shot,’ the newsreader announced from our black and white television set. Bobby Kennedy’s death happened on my father’s birthday. Like my dad, he was the father of a lot of children. We were Catholics, so were they. That evening, I walked down the passage from the TV room to the kitchen, sat at the yellow Laminex table on my own and ran my fingers along its surface. I often did this at meal times or while doing my homework. Its cool smoothness felt the same, but I didn’t anymore. This is what death can be, I thought. Your dad could die. My parents were sad too. We knelt and prayed for the Kennedys.
One of the prayers was the Hail Mary, with its gloomy last line, ‘Pray for us sinners now and at the hour of our death.’ I had learned that and other Catholic prayers by rote and they sat innocently enough among the jumble of nursery rhymes and verse poems like, ‘Ring a ring o’ roses, a pocketful of posies.’
Solemn or silly, it was soothing and fun to repeat them over and over. That they didn't make much sense didn't matter. Later in life, when I became interested in etymology and the genesis of individual words, I began to realise that true origins were often obscure, and meaning slippery. But back in 1960s Australia, it was simple and certain. For the Catholic tribe I was part of, God was in Heaven, our church was ‘the one true Church’, capital letters were very important, and if we were good children we would go to Heaven when we died.
—
When I finished school at seventeen I decided to do nursing, a job that would allow me to escape the small town I’d grown up in and work anywhere in the world. What I hadn't anticipated was that it would also make me a regular witness to the extremes of life — birth, death, great joy, deep suffering.
I moved to the city two hours away. Within days of starting my brand new career in a big hospital, I was kissed by a bikie with a broken leg and I had to wash and wrap a dead body.
In one of my first tasks, a senior nurse supervised me as I gave an unconscious patient a mouthwash. Standing next to the bed of an elderly lady, I held a moistened mouth swab and leaned towards her, poised, ready. The supervisor watched from the door — the woman had a contagious infection and anyone going into the room had to wear a protective gown and mask. But something wasn't quite right. I waved my swab-holding hand, signalling to the supervisor to come in. Irritated, she put on a mask, poked her arms into a gown, and came over to my side.
I stepped out of the way while she placed the back of her hand near the woman’s mouth to feel for her breath, then held the woman’s wrist. She shook her head. The old woman was dead. Briefly, I wondered if I’d done something to cause it. But there would be little time then, or later, for reflection, or questions, or answers.
‘I'll show you how to lie her flat, then we’ll talk to the charge sister about laying her out and who can help you,’ the supervisor said.
In a haze, I did my other jobs, waiting for someone to help me. Finally a nurse more experienced than me was free. Together we worked, standing on either side of the bed, reading through the instructions in the ward manual, washing the woman’s body in the order suggested.
By this time the old woman had been dead for several hours and as I wrote her name and hospital number in black Texta on her right leg — a task I particularly hated, and always would in the months and years after — I could feel the cool waxiness of her skin under my fingers.
The hospital had a standard issue large heavy-duty brown paper bag with a thin green strip through the centre, known simply as the clothes bag. I packed the old lady’s belongings into one, and left it on a chair next to the bed.
A little later, as I was crossing the corridor, running between patients, I saw an old man coming out of her room. He turned the corner into the long corridor and walked slowly to the exit on his own, gripping the clothes bag tight.
—
Through my twenties, I often looked after people who were dying and I was present at the moment of death for some.
One was an elderly woman, who lay in bed in a single hospital room, unconscious from a massive stroke the week before. Another nurse and I were attending to her, one of us holding her while the other smoothed cream over her back to keep her skin soft. The ward wasn’t busy and I decided to stay with her for a while.
The room was quiet, grey-white and spare. She had few possessions and no visitors. One nephew interstate was all the family she had left. He was fond of her, but the ties had loosened with the stretch of distance and he didn't want to leave his own family until there were more specific needs: a funeral to organise, her affairs to settle.
She lay on her side, one arm on top of the sheet, head low on the pillow, hair neat and tucked behind her ears. Her eyes were closed, her jaw loose, her mouth partly open. Her breathing was laboured, but soft. I sat by her bed, watching her, sometimes cupping my hand over hers, stroking her paper-thin skin with my fingertips. She looked comfortable.
After a time, she began to move. Her jaw lifted up, bringing her lips together. In one serene movement, she stretched her neck and straightened her head, took a deep breath and opened her eyes. She scanned the room, her gaze moving slowly from left to right. When her eyes met mine, she looked steadily at me, but at the same time through me, as if she was looking way beyond the walls. Her eyes completed an arc, she closed them again, her mouth relaxed and opened slightly, she stopped breathing, and died.
There was no obvious fear in the room, nor prayer or ritual. I sat there, aged twenty-four, spellbound. Her peaceful death was one thing; the vision she let me glimpse through her eyes something else. Of course I couldn’t know what had happened within her or what it might mean. In the quiet with her, with no disturbances or distractions, I experienced it as something both serious and light. A last glance at life, and she was off.
I had become more and more intrigued by the idea of a good death, and soon after that experience, I moved to England to specialise in palliative care, working in hospices there for a couple of years. One day I sat and watched in surprise as a similar thing happened with an old man. I had the sense that, like the old woman, he had looked a long way off, seen something that was alright, taken a deep last breath and let go.
—
It was around this time that I started thinking more about what being human is, beyond what my religious upbringing had suggested. Are we humans who have spiritual experiences from time to time? Or are we spirits having a human experience?
As I turned these questions around in my mind, a word that kept coming to me was ‘mystery’. Looking up its origins, I discovered it came from a Greek word which means both ‘to close the eyes or lips’ — as in, to keep secret — and ‘to initiate’.
Religious and spiritual people, philosophers, poets, writers and musicians regularly seek such initiation. Through the medium of their art, many became important companions to me as I worked with death and thought about life.
Poet and writer, Stephen Levine*, who worked with dying people for many years, has written a book about the year he spent living as if it were his last. Levine says that those familiar with the dying process, whether from experiences shared with the dying, decades of meditation, or moments of spontaneous grace, don’t speak of death as a single moment before which you’re alive and after which you’re not.
Instead they talk of a point of remembrance, when holding onto life transforms into letting go into death. In his view, ‘The heart never stops, for when it is no longer contained between opposing ventricles it expands slowly into its inherent vastness…expressing the truth it has embraced for a lifetime.’ From what I had glimpsed, in those years of sitting with dying people, and then washing and wrapping their bodies after death, this made sense to me.
In contrast to the mostly gentle transformations I saw in those years, I would sometimes think about how it might be for people who die violently. What happens for them in those final moments of life?
I recalled stories I’d heard about women who had experienced tremendous pain in childbirth and felt themselves leave their bodies, hovering above, watchful, until the pain had ebbed and their child was safely born. This gives me strange comfort. I can hope that those who die violently are able to leave their bodies, and the pain.
But doubts remain. Those spirits torn so abruptly from their experience of being human, are they reluctant to leave? Do they, for a time, try to get back?
—
I returned to Australia and continued to work in palliative care for a few more years, mostly with people who wanted to die at home. It was rich work, but tiring, and in my thirties I had a change, doing lighter work as a social policy researcher and writer. Then in my forties, it was time to think about death again.
‘Were you ever scared of me?’ my father asked me one day, after we had finished doing a shopping list. We were sitting side by side in two armchairs set up in his bedroom to accommodate the steady stream of visitors. Dad had cancer and was gradually sorting his sins. I saw pastoral care in action through the regular visits of his parish priest, a kind and decent bloke, who I imagined was prompting and helping Dad to make peace with himself and his god, and those of us orbiting close by.
‘Yes,’ I said.
‘Oh,’ he replied, looking surprised, hurt and relieved all at once.
Over the next few days, in between our different routines, there was a continuing conversation of words and thoughtful silences, about a difficult time when I was in my twenties, Dad in his fifties. We would share memories, go off and think about them, remember more, realise more, share more. We owed each other apologies, and the insights we both came by were a gift from the painful, honest talking that he started.
Dad lived eleven months from the time of his diagnosis, and died at home, as he had wanted. I was there much of the time, sometimes his nurse, mostly his daughter. Once, in the early stages, he asked me what the last days and weeks would be like, what he could expect. I took my mind back to hospice days and described the gradual ebbing of life I had often seen.
Months later, we were sitting side by side in the two armchairs, looking out the window of his bedroom at the trees, the creeper growing wild over the veranda railing. Dad said to me, ‘Remember you told me that the days would get shorter, and I’d sleep more.’
‘Yes,’ I said, as he lightly stroked the back of my hand with his fingertips. During those days, he sought touch much more.
‘It’s happening now, isn't it?’
I held my breath while my heart dived slowly, then turned itself around and settled back into my chest. Slowly breathing out, I said, ‘Yes, it seems to be happening now.’
He lay his head back on his chair, closed his eyes and said quietly, ‘It’s not too bad, is it?’
Later, when he was in bed all the time and knew death was close, Dad said: ‘Those poor fellows on the battlefields, dying alone, I wish they could have had someone with them too.’ Another time he talked about an Aboriginal man who had lived in the town with his young family, and whose wife had died in childbirth. Thirty years on, my dad’s sadness for him was still palpable.
His heart grew large as he was dying. He saw things differently, I know. I walked into his room one morning, a few days before he died, and he looked and smiled, and his face lit up with a deep honey-gold radiance that stopped me in my tracks. Without thinking, I said to him, ‘Where are you? What are you seeing?’
Physically weak, he couldn’t answer with words and now, years later, I wonder if it was wholehearted love that I saw on his face — love for me, and the rest of his big family, and soldiers alone on battlefields, and heartbroken Aboriginal men. I had thought he was seeing visions, but that sounds religious and his expression was totally alive and beyond religious imagery to me. I wonder if what he was seeing, and letting me see, was myself and all of us through an undefended, pure love, the opaqueness caused by a lifetime’s misunderstandings and missed opportunities fallen away in those moments.
On the day he died, Mum and several of us were with him, and his priest stood at the foot of the bed reciting the Hail Mary. ‘Pray for us sinners now and at the hour of our death.’ This was as Dad had wanted. I would have preferred silence though, and to touch his hand with my fingertips, as his heart unmoored itself and filled the sky.
—
After Dad died, I spent days and weeks in that strange place known as grief, trying to find him. I kept going back to the moment of his death, thinking that if I could just do one thing differently — what thing, I hadn’t yet worked out – he would come back, or still be here, or something. I was shocked by the completeness of his going. I had spent years working with dying people, and thinking about death and dying. Perhaps I thought it might inoculate me in some way.
A few weeks after his death, I went to the cemetery ten minutes’ drive away. Mum had a red rose bush in bloom by the side gate, and I picked one to take with me. I stood by his grave searching my brain, trying to work out what I was feeling, what I should be feeling, whether what I was feeling was what I thought I should be feeling.
Dad had a lovely wit and was always strong in a crisis. He could be uptight in a non-crisis, or make a crisis of something that wasn’t one, but he was definitely very calm, centred and strong when something truly awful was going on — his kids drinking kerosene, setting fire to car seats, choking on apple peel; Mum ill for a while. Around him in those times, I always had the sense that we would get through whatever it was that was happening, that it would all be alright.
These two qualities, his wit and calm lightness in the face of true difficulties, came to me this day, as I stood at his grave with my red rose, trying to be suitably sombre and meaningful. As I bent over to poke the stem in the dirt, I heard him speaking behind me. I knew he wasn’t actually there, but his presence was clear, his voice mischievous and loving as he said, ‘And rose from the dead.’ I cracked up laughing.
I still miss him, and did terribly for a time. Two years after his death, when his absence tore through me one day as I sat at my computer, alone in my home office, I wrote an email. ‘Some days I just hate it so much that Dad has died.’ It’s still there in the drafts box.
A while ago, an old friend came to stay with me on the eve of my fiftieth birthday. She meditates daily, kayaks and bush walks often and reads a lot. On my birthday morning, she woke me with a cup of tea and we sat side by side on my bed, talking. Feeling grateful for good friends, and that I’d made it this far, I said to her, my mood light, ‘So, what do you reckon it’s all about?’
Looking out the window at the big sky I can see from my upstairs room, she carved an arc in the air with her arm, gathering up the big expanse of the universe, and said she believes we are all part of this. Our form changes in cycles of life and death, but the essential self of each of us remains. Stars in the sky.
Australian composer Peter Sculthorpe, in his eighties* and still making beautiful music, has a simple take on life and death. He has said that he has no fear of death and death’s moment. ‘I don’t worry about it. I think, when we go, we sort of pass into some beautiful harmony of which we are part.’
We have dreams for love, for making a home, for making a difference, for making a beautiful life. What about a dream for death, for this important moment, in all its terrible beauty?
This piece was originally published in 2013. In the years since, author Stephen Levine passed away in 2016 at the age of 78 and composer Peter Sculthorpe passed away in 2014 at the age of 85. Nurse & Midwife Support extend our most sincere condolences to their loved ones and remember these talented artists for their important and beautiful work. Thank you, and rest peacefully.
If this piece has raised difficult feelings for you, we are here to talk. Call us on 1800 667 877 or email us.
About Lea McInereney
Lea trained as an RN and midwife in the early 1980s. She wanted to specialise in palliative care, which at the time was a new area of practice. The UK was a few years ahead of Australia, so she moved there for two years. First she studied oncology at London’s Royal Marsden Hospital, then palliative care at Sobell House in Oxford, under the clinical leadership of Dr Robert Twycross.
On her return to Australia, she worked in one of the many new palliative care services springing up. As the public became more aware of this different way of supporting people with advanced cancer, demand grew. More staff were needed and Lea discovered she had a knack for writing funding applications. The service grew rapidly and after some very busy years, Lea took a breath and made a sideways step into a health policy role. She’d always enjoyed writing (even the daily nursing notes on the wards!) and this new work involved lots of that. Lea also found that core nursing skills like observing, listening and problem solving were just as useful in the new job.
In the 1990s she did more study, this time in facilitation skills, and was mentored by several highly experienced facilitators and trainers. That led to a job in a staff development unit, where she ran courses in leadership and management skills.
In the 2000s, Lea left the public service and set up her own business as a facilitator and writer. Increasingly she was being asked by people to help them write complex policy documents in a way that would make them easily understood by the public. Her writing skills were pretty good, but she knew she could do it even better. She studied professional writing at RMIT for two years, adding ‘plain English specialist’ to her skill set.
The RMIT course also covered creative writing and Lea saw this as a great way to be able to tell important stories about health care and people’s lives. She’s now had a few stories and poems published. Two that come directly from her nursing experience are ‘Field Notes on Death’, the piece featured in this podcast, and ‘Routine Transfer (Maternity Ward, 1983).
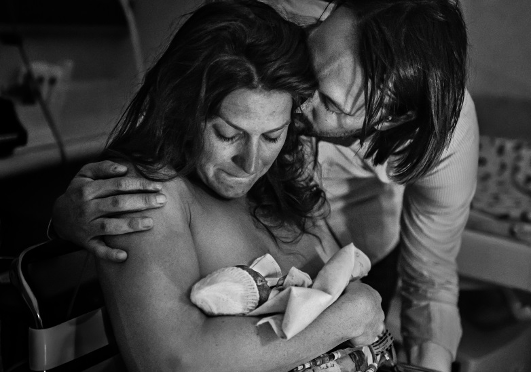
Photograph by Belle Verdiglione
Photographer Belle Verdiglione took this powerful photograph of parents Andrea and Franz with their stillborn baby girl Leia. The photograph was awarded 1st place in the Babies Born Still category at the 2019 Australian College of Midwives Birth Photography Awards.
Leia was delivered stillborn at 23 weeks after an infection spread to Andrea’s bloodstream. Leia was tiny, 635g and 28cm. Andrea described it to a journalist as a beautiful birth.
Andrea stayed with Leia in hospital for three days, giving the family time to hold her and say their goodbyes. In those days she spent time learning to crochet, lovingly creating a colourful jellyfish that would be cremated with her baby. Crocheting was her therapy, a ritual to focus her grief.
She has since continued to crochet jellyfish for babies in NICU and families around the world, also honours Leia through photography: “After coming home from hospital, I wanted to honour her memory and short life, and also do something for myself — create something I’m passionate about. That’s when I decided to pick up my long neglected hobby photography again. Photography is my therapy, so I’m only shooting what I’m passionate about and what makes me happy.”
Photography as therapy
Photography is a therapeutic tool for many families that experience stillbirths, premature births or have children with serious and terminal illnesses.
Photographer Belle Verdiglione had worked as a birth photographer for some time, but Leia’s birth was the first time she witnessed a baby ‘born sleeping’. She says that Leia’s birth forever changed her. She now volunteers with Hearfelt, an organisation that arranges professional photographers to work with grieving families.
Belle explains: “While I have close friends and family members who have experienced miscarriage and stillbirth, the stigma and silence that surrounds these families is deafening. I feel like we haven't moved with the times with this topic, it is still very much taboo, something to be hidden in the shadows, not talked about and for the families to grieve in silence. In an age where social media is very much a part of our everyday lives, stillbirth and infant loss is not visible.”
Improving Visibility
Photography is a way of making that grief and loss visible, celebrating the memory of their baby, and sharing their pain with others. The Australian College of Midwives Birth Photography Award for Babies Born Still is an acknowledgement of the incredible power sharing that memory can have.
At Nurse & Midwife Support, we thank Belle, Andrea, and Franz for sharing their story and beautiful photograph with us. Opening up the conversation around still birth and the challenging moments of being a midwife is really important.
If you have a story you’d like to tell, or would like a hand in debriefing, you can call us on 1800 667 877 or email us.
by Carole Arbuckle, NM Support Counsellor

A few years ago, I attended a wedding with some nursing colleagues. Although we only knew the groom, we were soon having a wonderful time dancing, singing and sharing funny stories. Suddenly, the groom’s father appeared beaming, saying; “You must be the palliative care nurses!” When I asked how he knew he simply said, “You seem to know how to enjoy life; it’s why I’m so pleased my son became a nurse…”
Professional witnesses to trauma
Nurses and midwives are professional witnesses to the worst moments in people’s lives. Many of us learn to be philosophical: we accept life can be tragically short. As a result, we strive to live life fully.
However, grief and loss can be unpredictable and complex. A philosophical approach is not always enough. We can experience significant and deep trauma as a result of grief and loss. We can carry personal grief into our professional lives. We can feel high levels of anxiety and inadequacy about what to say to clients who are wrestling with troubling and profound feelings about grief and loss.
Dealing with the struggle
Many of us struggle with this experience before we realise how to look at these issues. Self-care can be vital to manage and cope with grief and loss. Unfortunately, some of us might see self-care as just another thing we need to do at the end of a busy day.
The term self-care doesn’t suit everyone, so here’s a useful analogy: think of it as if you were going to rescue someone in a lake. You wouldn’t jump in if you couldn’t swim. You’d need to find resources, seek out appropriate assistance, and develop sound strategies and tools to support you. Otherwise, you’ll both drown.
Defining self-care
There are many definitions of self-care but here is my favourite:
True self-care is not salt baths and chocolate cake; it is making the choice to build a life you don’t need to regularly escape from
— Brianna Wiest
Like the clients I observed trying to adapt or accept the illness they were facing, I learned that the only way I could do the work I loved was to truly adapt and accept that self-care was vital and understand how to make positive choices to maintain it. Initially, it wasn’t easy. At the time, I believed nurses should push through, and we should be able to cope quietly, invisibly — without help.
I was wrong. Now, I choose to accept I am not immune to the impact of grief and loss in my professional and personal life. I choose to give myself permission to talk to someone I trust when I feel affected by grief and loss. I accept I am potentially susceptible to burnout or compassion fatigue. In fact, I now understand this is common, especially if you didn’t know the signs and your personal triggers. I chose to learn what those were.
Finding the right tools
Over time, I also learned that I could develop cognitive and emotional tools and knowledge that gave me permission to say: I do not have special powers. It’s OK to be a ‘work in progress’ but still strive to be a valuable support to clients. I choose to accept vulnerability as an important part of being deeply human for ourselves and our clients. This sensitive, intricate, fragile and vital part of us serves as an important way to grow and make our lives more satisfying, richer, fuller and meaningful.
It doesn’t happen overnight
It’s important to note: I didn’t wake up one day with these realisations. My experience is a lifelong approach, a collective ongoing process — seeking out education on grief and loss, learning to recognise burnout and compassion fatigue, building informal networks with trusted peers who are prepared to be honest, open and vulnerable.
Counselling was incredibly helpful to unpack the unconscious processes and motivations that underpinned my professional life, both positively and negatively. Interestingly, psychologists and psychiatrists use this method for psychological support and safety, yet nurses and midwives, who are intimately involved with loss and grief at every part of our client’s lives from birth to death, largely do not. Our service can help with this call for a debrief anytime on 1800 667 877.
Strong social connections are paramount. It is crucial to be like the palliative care nurse friends I mentioned at the beginning of this blog, striving to live life fully with people who you enjoy and who enjoy you. Making conscious choices about coping with loss and grief sustain you to do the work we do safely and rewardingly — in short, make choices that don’t make you feel like you’ve built a life you regularly need to escape from.

In Mexico and other parts of Latin America, people build altars to remember lost loved ones on Dia De Los Muertos (Day of the Dead). This holiday celebrates life and death with colour, delicious food, and dancing.
Note: this podcast was recorded before the escalation of COVID19 which is why we don’t specifically mention it.
Nurses, midwives and students navigate the complexities of caring for people while dying, in death and while grieving. Sometimes, we have to remind ourselves that we are not immune from the effects of grief, compassion fatigue and vicarious trauma.
I discuss those effects with guests Lea McInerney and Carole Arbuckle in this new episode of our podcast. I have called this the STORY podcast: nurses and midwives have many stories related to caring for people who are dying and supporting the grief of those around them — sometimes their own grief. In this episode we share our stories.
My guests Lea and Carole have many years of experience as palliative care nurses.
Lea trained and worked as a nurse and midwife who now works in policy with the Department of Health. She wrote and first published Field Notes on Death in 2013. We were so touched by this beautiful and poignant memoir of witnessing and caring for people while dying and in death that we included it in the Autumn 2020 edition of our newsletter.
On the podcast, Lea shares the story of writing this heartfelt piece and discusses the importance of taking care of ourselves when we care for others, and creating space in our lives to deal with grief.
Carole is an experienced RN who has 25 years’ experience in oncology and palliative care. Her main passions have been communication and cancer. Carole is now a nurse clinician with Nurse & Midwife Support. Carole shares her career journey working in cancer care and palliative care and recalls an important insight she gained from a young boy as she cared for his dying father.
Carole outlines why it is important for all nurses and midwives to reach out for support if they are troubled or challenged by their work. She also wrote this wonderful companion piece ‘How to enjoy life in the presence of death’ about dealing with drama and trauma in a helpful way and how to look after yourselves.
Carole and Lea believe that it is time nurses and midwives told their stories as in their telling we heal, learn and grow. All OUR STORIES MATTER.
It was my pleasure and privilege to talk to these inspiring experts.
Mark Aitken RN
Stakeholder Engagement Manager
Nurse & Midwife Support
Listen to the podcast and read the transcript
For confidential advice and support you can contact us at 1800 667 877 or emergency support 24/7